
Dr Jimoh Olubanwo Agbaje¹, Dr.Henri Diederich*²
1. OMFS-IMPATH Research Group, Department of Imaging and Pathology, Faculty of Medicine, Catholic University Leuven, Belgium
2. Dr.Henri Diederich, 114 av de la Faiencerie, L- 1511 Luxembourg
Corresponding Author: Dr. Henri Diederich, Medical Doctorate in Dental Public Health SMSB- SUDAN
CopyRight: © 2022 Dr. Henri Diederich, This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Abstract
The method by which prosthesis are connected to implant components (e.g Abutment) plays a major significant role in the the clinical success of the restoration. Cement and screw method of prosthesis retention have both advantages and limitations. Combining both methods of restoration ( i.e. screw and cement-retained restoration) benefits from the advantages of both methods
The following case reports illustrate procedures where atrophied edentulous jaws were treated using a minimally invasive method and the restorations were retained with screw and cement.
Keywords: implant prosthesis, one piece implants, pterygoid implants, one piece tissue level implants, dual retention, retrievability
Introduction
The method by which prosthesis are connected to implant components (e.g Abutment) plays a major significant role in the the clinical success of the restoration. The strengths and weaknesses of each retention method should be considered and tailored towards each individual clinical situation of the patient1-6.
The component retention can be achieved by screw-, friction-, or cement-retention or combined screw and cement retention. The choice of retention methods are usually determined by retrievability, stress, esthetics, and accessibility7.
Cement retention is often considered to be the most successful method by reducing stress in the restoration and bone, excess cement application leading to bone loss and peri-implant disease are major issues. Patient dissatisfaction due to repeated loosening of the prosthesis cause by debonding is also a major issue in cement only retained restorations2,8-10.
Screw-retained restorations allow for easier removal and access for maintenance, however, achieving a passive fit is significantly more difficult to attain with a screw-retained restoration due to stress introduced into the restoration through the tightening of screws10,11.
The dual retained restorations ( i.e. screw and cement retained restoration) combine the advantage of both screw and cement retained restorations8-10,12. A thin layer of the cement reduces stress in the restoration and also compensate for any minor discrepancies in the fit. Further Cement-retained restorations reduce stress and the likelihood of stress related implant failure or peri-implantitis. The use of temporary cement makes restoration removal easier.
Screw-retained implant reconstructions are easier to remove for maintenance, repairs, or when surgical interventions when required8,10. The retention screw used at a pterygoid implant of the posterior maxilla offers an additional strong anchorage in a fixed prosthesis. The telescopic ones were luted with temporary cement in order to avoid food leakage and microbial colonization. The restoration could be easily retrieved if the retaining screw was removed10,11.
Many previous articles have described the clinical procedure for the restoration of severely resorbed jaws (maxilla and mandible) with cortically fixed implant system13-16. Cortically Fixed at Once approach has been shown to be a reliable alternative to bone grafts and sinus lift in situations where there is a substantial bone resorption. The surgical technique as well as the laboratory procedures has been well elucidated15-17.
The following case reports describe procedures where atrophied edentulous jaws were treated using a minimal invasive method and the restorations were retained with both screw and cement.
Case reports
A 54 year old male patient wanted fixed teeth in his maxilla. He presented at the clinic with a reason to get fixed teeth in the maxilla. A clinical examination of the mouth showed a partial edentulous lower and upper arch with resorbed ridge and periodontally compromised teeth 14,16 and 26. Radiographic examination using an orthopantomogram showed a partial edentulous upper jaws with moderate vertical bone resorption in the front and severe vertical resorption in the premolar and molar region (Figure 1).

Figure 1: Panoramic radiograph of the patient at pre-treatment showing partially edentulous upper arch with resorbed alveolus bone and remaining teeth
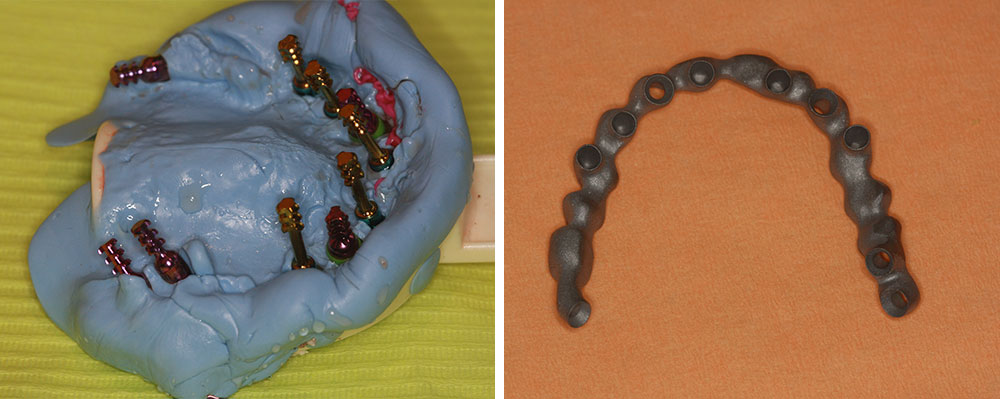
Figure 2: Laboratory steps. Impression after surgery and frame fabrication
Treatment Plan: From a prosthetic point of view, the patient desired a fixed prosthetic solution. In the upper jaw a minimal invasive procedure, One Piece Compressive Implants (Cemented temp bond) and One Piece Tissue Level screw retained Implants were used, (ROOTT-Implants, Trate AG).
Immediate loading treatment with a metal-ceramic bridge was proposed. The patient agreed to this treatment plan. The pre-treatment situation of the patient is shown in figure 1.,
After implant placement, the surgery, transfer copings were screwed on both types of tissue-level Implants. Friction fit transfers were placed on the One Piece Implants. ts. The bite was registered at the same session. At the second appointment, the frame was tried and the occlusion was reviewed again.
Two weeks after the surgery the metal-ceramic bridge was delivered and fixed to the patient,s jaw with both screw and cement-retained (Temp-bond) fixations.
The above restoration was done with One Piece Compressive Implants (Cemented with temporary bond) and One Piece Tissue Level screw retained implants.

Figure 3: Panoramic radiograph of the patient after prosthesis delivery

Figure 4: Panoramic radiograph of patient pre-surgery
In figure 3, the One Piece Implants in position 15 and 25 were bent (3.5,16mm)This type of rehabilitation with a One Piece Compressive implant is less invasive than using Cortical Hybrid- Plates implants at the zygomatic arch.
The Cortical, Hybrid Plates are usually used when One Piece Implants are not appropriate due to a weak bone.
In a similar case a male patient in good health wanted fixed prosthesis in the maxilla . The patient did not want any invasive surgical operation like sinus lift or bone grafting. The figure below shows the panoramic radiograph of patient at pre-surgery.
The agreed treatment option was extraction of all remaining teeth in the maxilla and implant placement using pterygoid implants, one piece compressive Implants (Roott, Trate Ag), and one piece tissue level screw retained implants.
After implant placement surgery, a bite registration was done. Then transfer copings were placed and an impression was taken with silicone immediately after the surgery. One week later the try-in (figure 5) an appointment for prosthesis delivery was given.

Figure 5: Clinical photograph of a) frame and b) frame try in

Figure 6: Soft tissues of the maxilla before bridge placement

Figure 7: a) Metal-ceramic bridges and b) clinical photo of the patient with the restoration in the mouth
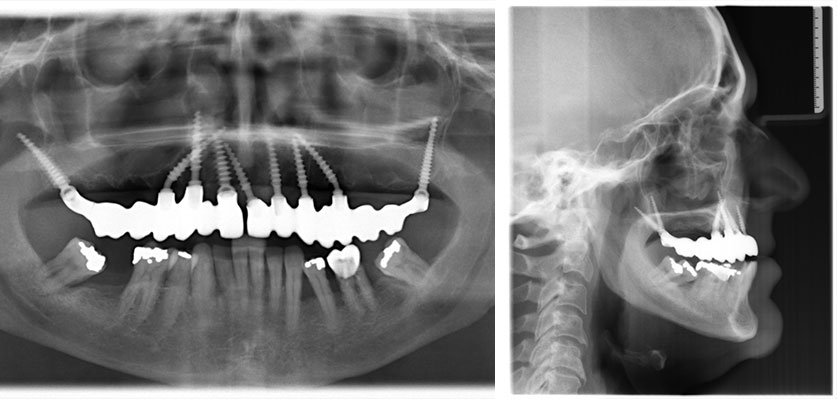
Figure 8: a) The panoramic and b) lateral cephalometric radiograph of the patient at completion
The definitive metal-ceramic bridge was cemented and screwed, the ceramic bridge was delivered after 2 weeks.
The following case was a 75-year-old lady, she wanted to replace her broken bridge in the maxilla. She had a previous experience with flapless implant placement and immediate loading in the mandible 7 years before. Due to her positive experience she wanted the same treatment for the maxilla.
In the maxilla, One piece Compressive implants were placed (Roott,Trate ag) in the anterior region and Pterygoid implants (Roott, Trate Ag) for the posterior anchorage. Try- in of the frame was done after 6 days. The finished metal-ceramic bridge was delivered 2 weeks later. The new metal-ceramic bridge was cemented on the One Piece Implants and screwed on the one piece tissue level and pterygoid implants ten days later. The finished work is presented in figures 11 and 12.

Figure 11: Shows the clinical photo of a) the metal-ceramic bridge and b) patient with metal-ceramic bridge in the patients mouth
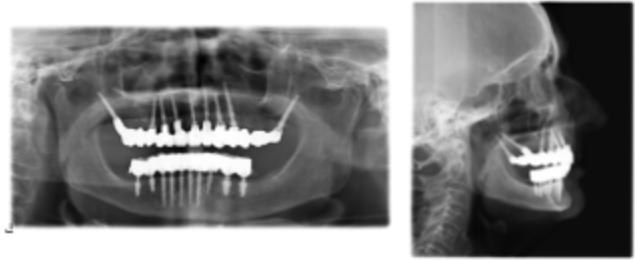
Figure 12: a) The panoramic and b) lateral cephalometric radiograph of the patient at completion
The last patient in this series is a 88 year old patient with a loose bridge who wanted new fixed restoration. The panoramic radiograph of patient at presentation is shown in figure 13. The treatment option was extraction of the teeth with loosen bridge and implant placement with immediate loading. The finished metal ceramic bridge was cemented (temp-bond) after 2 weeks. Figure 15 shows the clinical and panoramic radiograph of the patient after treatment. A fast and efficient treatment option is important especially for elderly patient like the one presented here, Also in this case as shown in Fig 15 the one piece compressive Implants were bent (as seen in the radiograph) to avoid injury to the mandibular nerve, as in the maxilla it may avoid sinus-lift.

Figure 13: Panoramic radiograph of patient at presentation

Figure 14: One-piece compressive implants
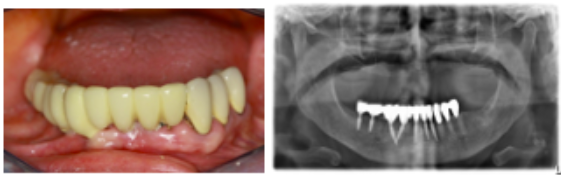
Figure 15-16: Clinical photo; Panoramic radiograph of patient at presentation
The presented case reports describe the functional restoration of edentulous patient and partial edentulous patient with atrophied jaw who do not want additional surgical procedure such as sinus lift and bone grafts. All cases presented above were done with a minimal invasive technique and immediate loading, the prosthesis were cemented and screwed.
In some of the cases bent one piece compressive Implants were used , this is less invasive and in some cases prevent nerve injury (figure 16).
In all cases, the patient problem of edentulism in the jaw could be solved without additional surgical procedures. The procedure is fast, less invasive with a minimum of components. The short treatment time leads to a happy patient as their oral problems can be solved within a short period.
Previous review published by the authors of cases treated with combined, cemented and screw retained prosthesis of more than 15 years has shown the long-term success of this method of prosthesis retention.
References
- Hebel KS and Gajjar RC. Cement-Retained Versus Screw-Retained Implant Restorations: Achieving Optimal Occlusion and Esthetics in Implant Dentistry. J Prosthet Dent 1997; 77: 28-35.
- Chee W, Felton DA, Johnson PF, Sullivan DY. Cemented Versus Screw-Retained Implant Prostheses: Which Is Better? Int J Oral Maxillofac Implants 1999; 14: 137-141.
- Cordaro L, Ercoli C, Rossini C, Torsello F, Feng C. Retrospective Evaluation of Complete-Arch Fixed Partial Dentures Connecting Teeth and Implant Abutments in Patients With Normal and Reduced Periodontal Support. J Prosthet Dent 2005; 94: 313-320.
- Proussaefs P and AlHelal A. The Combination Prosthesis: A Digitally Designed Retrievable Cement- and Screw-Retained Implant-Supported Prosthesis. J Prosthet Dent 2018; 119: 535-539.
- Rues S, Kappel S, Ruckes D, Rammelsberg P, Zenthöfer A. Resistance to Fracture in Fixed Dental Prostheses Over Cemented and Screw-Retained Implant-Supported Zirconia Cantilevers in the Anterior Region: An In Vitro Study. Int J Oral Maxillofac Implants 2020; 35: 521-529.
- Malpartida-Carrillo V, Tinedo-López PL, Ortiz-Culca F, Guerrero ME, Amaya-Pajares SP, Özcan M. Fracture Resistance of Cement-Retained, Screw-Retained, and Combined Cement- and Screw-Retained Metal-Ceramic Implant-Supported Molar Restorations. J Contemp Dent Pract 2020; 21: 868-873.
- Thalji G, Bryington M, De Kok IJ, Cooper LF. Prosthodontic Management of Implant Therapy. Dent Clin North Am 2014; 58: 207-225.
- Preiskel HW and Tsolka P. Cement- and Screw-Retained Implant-Supported Prostheses: Up to 10 Years of Follow-Up of a New Design. Int J Oral Maxillofac Implants 2004; 19: 87-91.
- Song T, Xu PC, Li Y. [Clinical Observation of Screw and Cement-Retained Implant-Supported Restoration of Fixed Bridges]. Shanghai Kou Qiang Yi Xue 2011; 20: 296-299.
- Spazzin AO, Camargo B, Bacchi A. Ensuring Passivity and Retrievability for Immediate Complete-Arch Implant-Supported Prostheses. J Prosthet Dent 2017; 117: 214-217.
- Malpartida-Carrillo V, Tinedo-Lopez PL, Ortiz-Culca F, Guerrero ME, Amaya-Pajares SP. Techniques for Retrievability and for Registering Screw Access Holes in Cement-Retained Implant-Supported Prostheses: A&Nbsp;Scoping Review of the Literature. J Prosthet Dent 2020; 123: 427-433.
- Chee WW, Torbati A, Albouy JP. Retrievable Cemented Implant Restorations. J Prosthodont 1998; 7: 120-125.
- Agbaje JO, Diederich H. Rehabilitation of Atrophic Maxilla Using Pterygoid Implants: Case Reports. 2018.
- Agbaje JO, Diederich H. Minimal Invasive Modality for Full Rehabilitation of Edentulous Mandible With One-Piece Implants in Elderly Patients; A Case Report. 2018.
- Agbaje JO, Diederich H. Use of Cortically Fixed at Once Implants for the Treatment of Atrophic and Extreme Athrophic Jaws. 2018.
- Agbaje JO, Diederich H. Cortically Fixed at Once Implants for the Treatment of the Atrophic Maxilla – A Case Report. 2019.
- Agbaje JO, Diederich H. Minimal Invasive Concept for the Rehabilitation of Edentulous Jaw With One-Piece Implants. 2018.